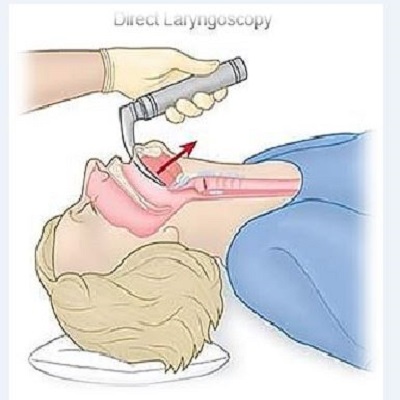

Direct laryngoscopy
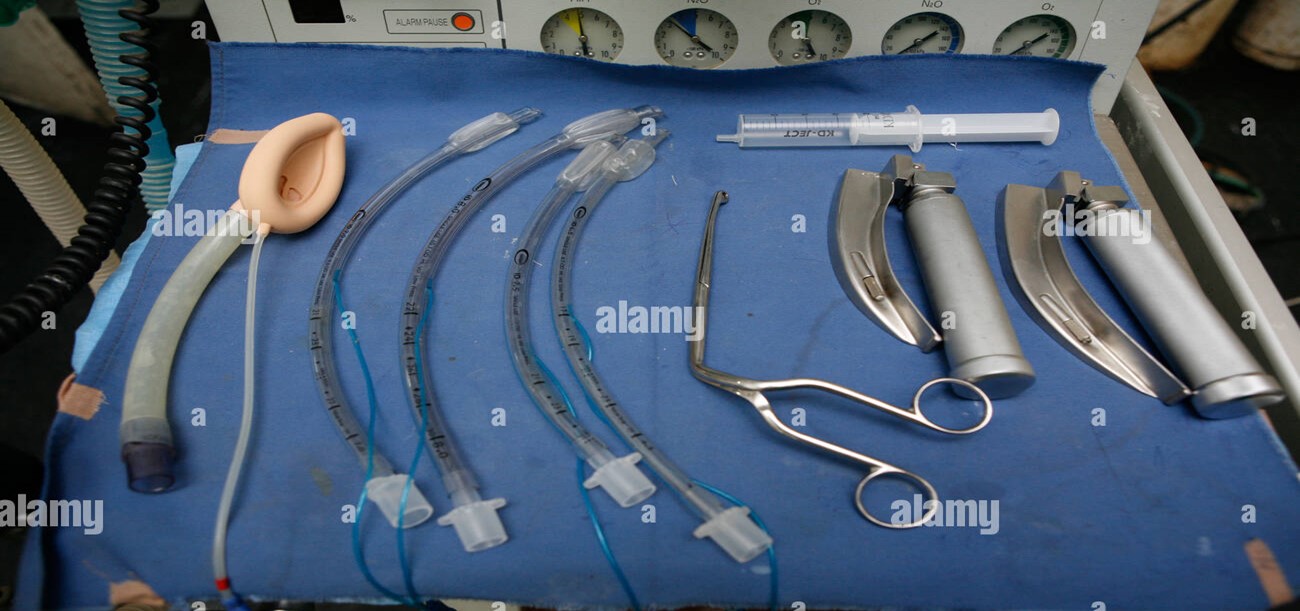
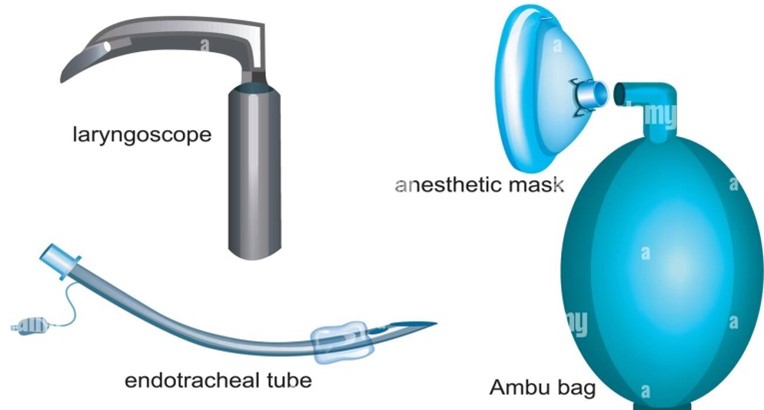
A direct laryngoscopy allows visualization of the larynx. It is used during general anesthesia, surgical procedures around the larynx, and resuscitation. This tool is useful in multiple hospital settings, from the emergency department to the intensive care unit and the operating room. By visualizing the larynx, endotracheal intubation is facilitated. This is an important step for a range of patients who are unable to secure their own airway, including those with altered mental status and those who are undergoing a surgical procedure. When using direct laryngoscopy to secure a patient's airway, the physician must be well acquainted with the anatomy, indications, contraindications, preparation, equipment, proper technique, personnel, and complications of the procedure for successful endotracheal intubation.<br />Anatomy and Physiology<br />The larynx is situated just below the pharynx. It is comprised of three paired smaller cartilages, three unpaired cartilages, and the intrinsic muscles. The three paired cartilages include the arytenoids, corniculate, and cuneiform. The three unpaired cartilages include the cricoid, thyroid, and epiglottis. The cricoid cartilage is the only cartilage that covers the circumference of the trachea. The epiglottis, which is superior to the cricoid cartilage, is an important landmark for direct laryngoscopy. The epiglottis is located at the base of the tongue and encapsulates the glottis to form a lid over it. The epiglottis protects the larynx from the aspiration of gastric contents. At the base of the tongue, anterior to the epiglottis is a pocket of cartilage known as the vallecula. The vallecula is an equally important landmark, as certain types of direct laryngoscopy blades, such as the curved or Macintosh blade, are inserted into order to manipulate the area to improve visualization of the vocal cords. When the laryngoscope blade is in the vallecula, it is pressed up against the hyoepiglottic ligament, which suspends the epiglottis from the hyoid bone.<br />Indications<br />Direct laryngoscopy to perform endotracheal intubation is indicated in the emergent setting in perioperative settings or the intensive care setting. In the emergency room, the indications for direct laryngoscopy to perform endotracheal intubation include acute respiratory failure, impending airway collapse indicated by hypoxia or hypercapnia, and airway protection in patients with altered or depressed mental status, upper gastrointestinal bleeding or hematemesis secondary to bleeding from esophageal varices. In the perioperative setting, endotracheal tubes can be placed using direct laryngoscopy for patients receiving general anesthesia, surgeries involving the airway or areas adjacent to it, or surgeries involving unusual positioning, such as spinal surgery, which requires prone positioning. In the intensive care unit, direct laryngoscopy for endotracheal intubation is performed for impending airway collapse, or short-term hyperventilation of patients with increased intracranial pressures in the setting of intracranial hemorrhage, tumors or masses. Intubations in the intensive care unit are also performed to manage copious secretions.<br />Contraindications<br />Direct laryngoscopy has few absolute contraindications. Such absolute contraindications involve supraglottic and glottic lesions that would prohibit the advancement of the endotracheal tube (ETT) such as high-grade subglottic or glottic stenosis or complete obstruction by supraglottic or glottic tumors. Additionally, blunt trauma to larynx resulting in laryngeal fracture or disruption of the laryngotracheal junction can become worse in the setting of traction from laryngoscope blade, placement of the ETT or pressure from the ETT stylet, which can promote the creation of a false lumen in the trachea or cause perforation through the trachea. In these patients, a surgical airway is required.<br />Direct laryngoscopy for ETT placement is also contraindicated in the case of penetrating trauma to the upper airway, in which manipulation of the area by laryngoscope or ETT may cause a hematoma, partial or complete transection of the airway. In such suspected cases, ventilation and oxygenation should be accomplished via non-invasive means until a definite surgical airway is established.<br />Grade III trismus (inter-incisoral distance of <1 cm) is an absolute contraindication to direct laryngoscopy, though, in practice, direct laryngoscopy is rarely possible with grade II trismus either.<br />Relative contraindications to laryngoscopy include difficulties in performing the procedure, such as patients with difficult airways (i.e., micrognathia, macroglossia, high Mallampatti score), injury, and trauma of the neck, pharynx, or larynx. In addition, patients with airborne diseases who require their airway secured, for example, those with Tuberculosis, COVID19, Ebola, to name a few, should not undergo direct laryngoscopy if possible due to transmission of the pathogen to healthcare personnel.<br /><br /><br /><br />Equipment<br />1- Laryngoscope Handle (power source)<br /> Blade (light source)<br />2- Endotracheal intubation<br />3- Ambuo-bag<br />4- Stylet<br />5- Stethoscope<br />6- Syringe <br />Learning objective<br />• Identify the anatomical structures visualized during direct laryngoscopy.<br />• Describe the technique of direct laryngoscopy.<br />• Review the indications of direct laryngoscopy.<br />• Explain inter-professional team strategies for improving care coordination of patients undergoing direct laryngoscopy and improving outcomes.<br />7- Magill's forceps<br /><br />By: B.M.T. Nada shaker