تلوين الغدد اللعابية......... كرار حيدر عبد الحسين
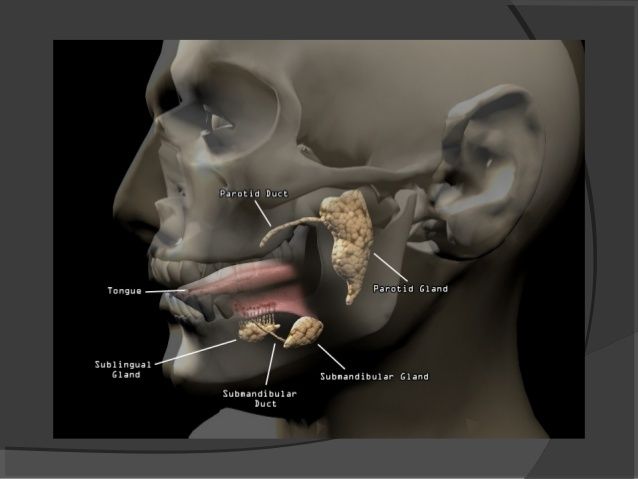
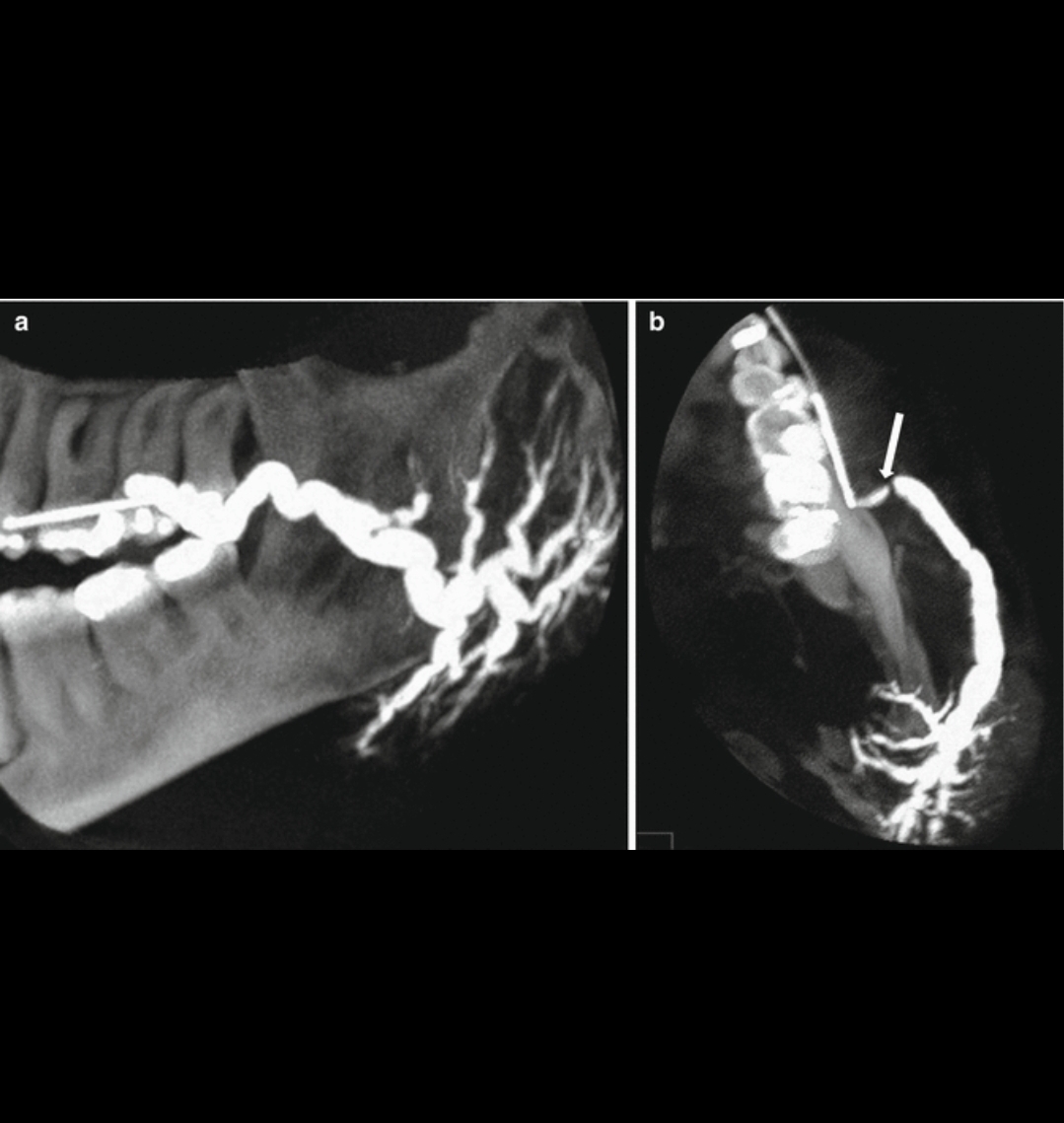
Sialography<br />INDICATIONS <br />1. Calculi.<br />2. Chronic inflammatory disease.<br />3. Mass lesion.<br />4. Obstructive lesion.<br />5. Penetrating trauma.<br />6. Strictures.<br />7. Fistula.<br />8. Prior to CT evaluation of salivary glands.<br /><br />CONTRAINDICATIONS <br />1. Allergy to iodine.<br />2. Acute Sialadenitis.<br /><br />EQUIPMENT <br />1. Contrast medium-water soluble, ionic contrast media like<br />Triovideo 280,Conray 280 or non-ionic contrast medium such as<br />omnipaque-350.<br />2. Lacrimal cannula or disposable 22 G (Gelco/Venflon).<br />3. Lacrimal dilator. Liebreich's double ended lacrimal probe.<br />4. 2 cc syringe. Four grades (00/0, 1/2, 3/4 & 5/6) 00/0 and ½<br />are required for sialography. Outer diametre of cannula 1.02 mm.<br />Rabinov sialography catheter obtainable in a sterile pack and is<br />recommonded.<br />5. Lemon/vitamin C tablet.<br /><br />PROCEDURE <br />l. Preliminary radiograph<br />Plain radiograph should be taken before embarking on sialography<br />because a considerable pathology is associated with opaque calculi<br />within the glands themselves or their ducts, particularly in the<br />submandibular gland.<br />2. Locating duct openings<br />(a) Parotid duct opens opposite 2nd upper molar tooth on the<br />buccal surface of the cheek.<br />(b) Submandibular duct opens at the base of the frenulum of the<br />tongue.<br />(c) In case the ostium is not visible, apply pressure on the gland<br />or give a sialogogue like lime. Then saliva will be seen pouring<br />through the punctum.<br />3. Dilate the punctum with lacrimal dilator.<br />4. Technique<br />Two techniques for cannulating the ducts are by using:<br />(a) Intracath technique.<br />(b) Lacrimal cannula technique.<br />• If we are using an intracath, we should cut enough plastic<br />tubing from the tip of intracath with fine scissors such that<br />2 mm of the inner wire stilette is still protruding. Now the<br />punctum is cannulated for 5 mm. Now withdraw the stilette<br />such that it no longer protrudes the outer tube.<br />• The inner stilette produces stiffness during introduction of<br />catheter. The stilette is removed and outer tube is attached to<br />polythene tube.<br />• Now the contrast is injected.<br />• In the lacrimal cannula method, contrast is injected into the<br />cannula which is introduced through the duct opening<br />• Contrast is injected till the patient complains of pain by a<br />prearranged signal.<br />• About 0.5-1.0 cc of contrast is required.<br />5. Film exposure<br />Positioning for parotids:<br />• Frontal view is taken with face rotated 5-10 degrees towards<br />the side of study.<br />• Lateral view is taken with 15-20 degrees cranial tube tilt.<br />Positioning for submandibular gland<br />• Lateral view is taken with 15-20 degrees cranial tube tilt.<br />Films are taken during injection. The catheter is left in place<br />till the adequacy of films is ensured.<br />6. Aftercare: none<br />If sialadenitis occurs after the procedure, it should be treated with<br />antibiotics and anti-inflammatory drugs.<br />7. Complications<br />• Sialadenitis and abscess<br />• Stricture of the ducts.<br />8. Disadvantages of sialogram<br />• Masses less than 1cm may not be detected.<br />• Contrast does not always penetrate the deep lobe of parotid<br />gland.<br />