Advances in Regional Anesthesia For Shoulder Surgery
11/02/2022 Share :
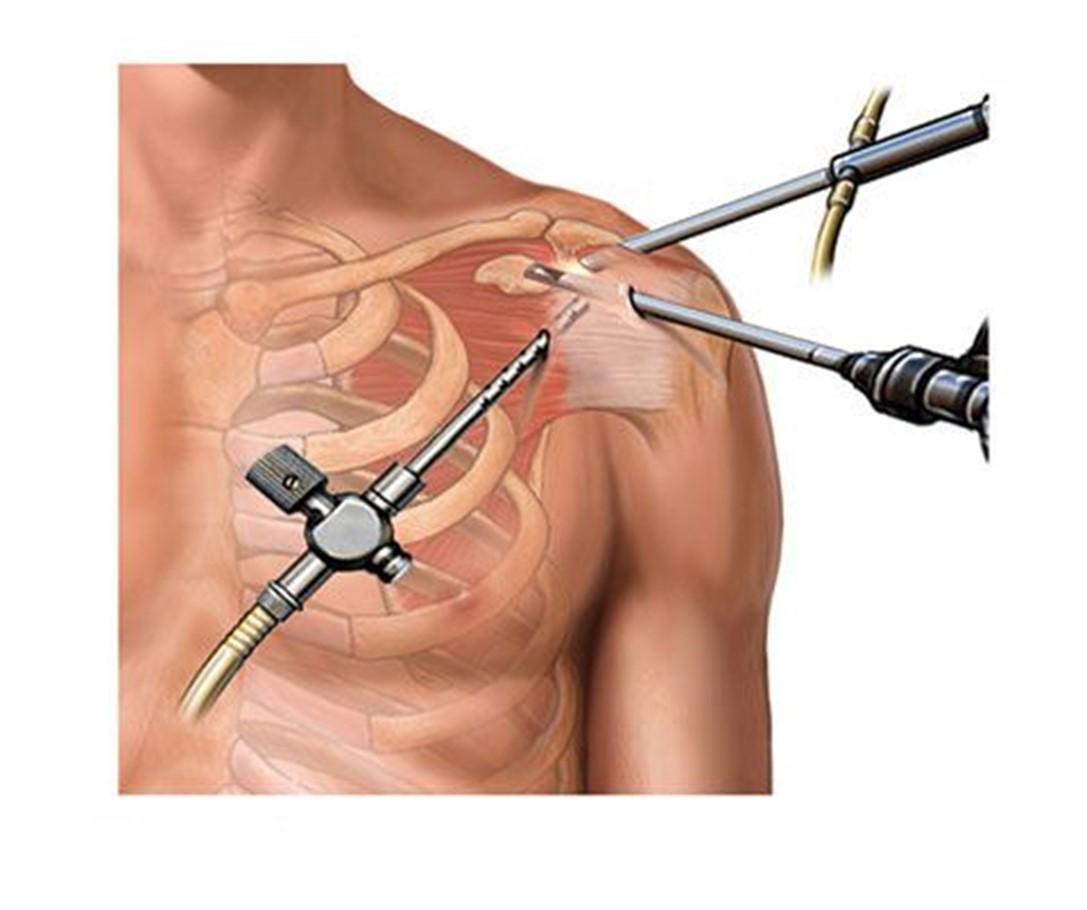
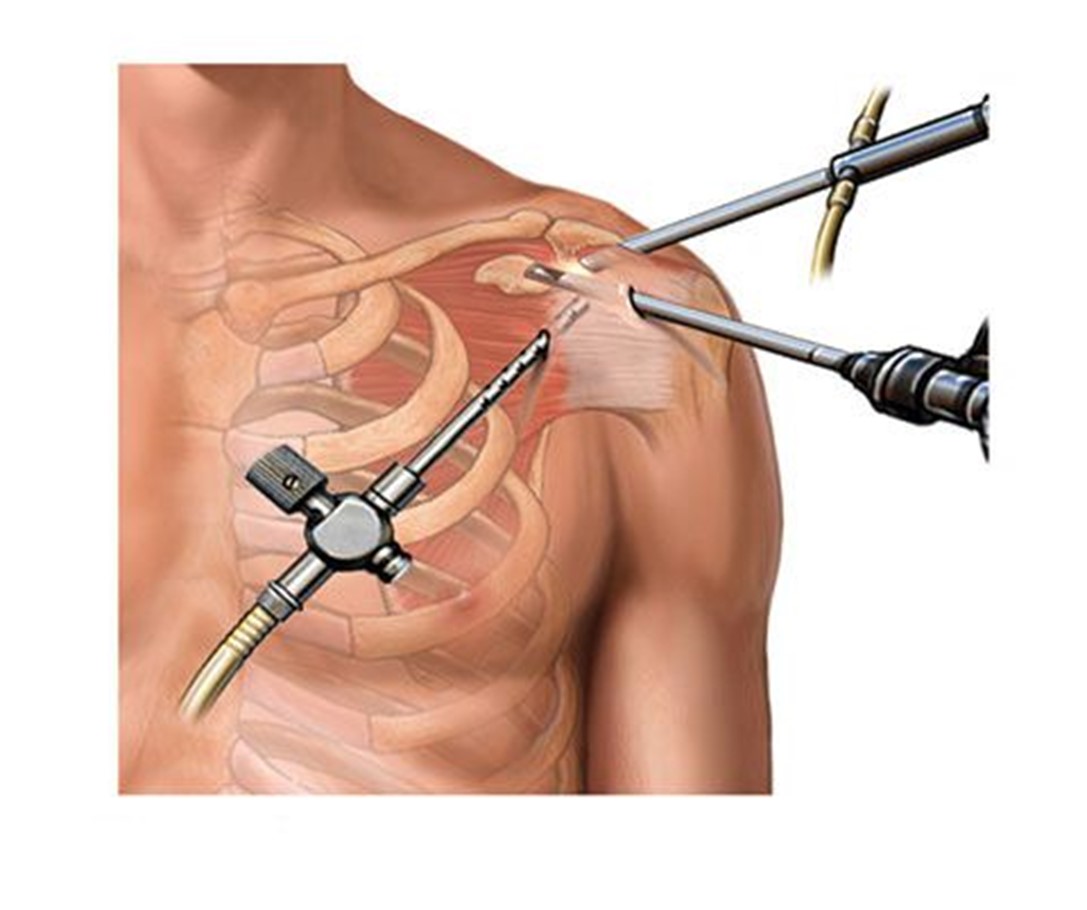
The prevalence of shoulder pain in the population is 7% overall, increasing to 26% in those aged >70 yrs.<br /> Acromioplasty (sub-acromial decompression), stabilisation, adhesiolysis (release of frozen shoulder) and rotator cuff repair are the most common procedures undertaken, and these are usually performed arthroscopically. <br />Open procedures include arthroplasty of the glenohumeral joint, which can be performed as a total or partial joint replacement, open stabilisation, open rotator cuff repair, and most trauma procedures.<br />shoulder surgery generally results in significant postoperative pain requiring opioids, regional anaesthesia forms an important part of the anaesthetic technique by improving patient experience, reduces operating theatre time, and reduces postoperative complications such as pain, sedation, nausea, and vomiting, and the need for overnight stay.<br /> Regional anaesthesia can be used as a sole anaesthetic technique or it can be combined with general anaesthesia.<br /><br />For decades, interscalene brachial plexus has been the gold standard; however, a significant number of patients develop hemidiaphragmatic paralysis (HDP) due to unilateral phrenic nerve blockade sometimes requiring respiratory monitoring. This is particularly important in patients with severe pulmonary disease and obese individuals. Lowering the local anaesthetic volume and deposition lateral to the brachial plexus is an attractive alternative, but this does not completely eliminate the risk. Other investigators have suggested a combination of supraclavicular brachial plexus approach with suprascapular nerve block. <br />infraclavicular block in combination with suprascapular nerve block (to cover the posterior aspect of shoulder joint<br />costoclavicular approach to brachial plexus has been described. Cadaver studies reveal that the three cords lie in close proximity lateral to axillary artery and vein in a triangular fashion in the costoclavicular space, which is located deep and posterior to the midpoint of the clavicle. Although the benefits of this approach are similar to supraclavicular block, the risk of pneumothorax and sparing of lower trunk nerves is lower. This block is particularly useful for vascular, wrist and hand surgeries. <br /><br />By Dr. Mohammed Sami Hassan