
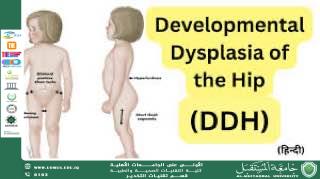
Developmental Dysplasia of the Hip (DDH) — Formerly Known as Congenital Dislocation of the Hip
The term “Developmental Dysplasia of the Hip” (DDH) is preferred over “congenital” because the condition may be present at birth or may develop during the first weeks or months of life. DDH is a treatable condition, and early detection is the most important factor for achieving a successful outcome. For this reason, pediatricians routinely screen the hips at each well-baby visit during the first year.
What Is DDH?
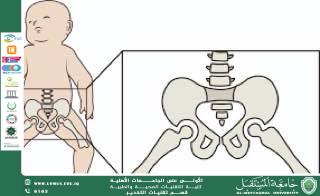
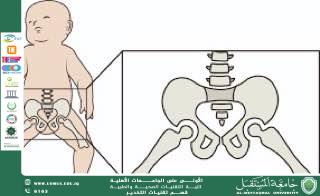
DDH is a condition in which a baby’s hip joint does not form properly. It represents a spectrum ranging from a shallow acetabulum to partial (subluxated) or complete dislocation, due to instability of the femoral head within the socket. This instability interferes with normal hip development.
Severity Spectrum
1. Dysplastic Hip: Shallow socket but the femoral head remains in place.
2. Subluxatable Hip: The head is in the socket but can be partially displaced on examination.
3. Dislocatable Hip: The head is in the socket but can be pushed out with a maneuver.
4. Dislocated Hip: The femoral head is completely out of the socket.
Causes & Risk Factors
The exact cause is unknown, but genetic and environmental factors are believed to contribute.
• Breech position (strongest risk factor, especially in girls)
• Family history of DDH
• Female gender: 4–6× higher risk due to ligamentous laxity
• Firstborn infants: limited intrauterine space
• Oligohydramnios: reduced fetal movement
Signs and Symptoms
In Infants
• Asymmetric thigh or buttock skin folds
• Limited hip abduction
• Positive Ortolani or Barlow signs (performed only by a physician)
• Apparent leg-length discrepancy
In Older Babies or Children
• Delayed walking
• Limping (unilateral) or waddling gait (bilateral)
• Toe-walking on one side
Diagnosis
• Physical examination: initial screening tool
• Ultrasound: gold standard under 6 months
• X-ray: useful after 4–6 months
• MRI: may assist in early or complex cases
Treatment
Birth to 6 Months
• Goal: stable, flexed, abducted position
• Pavlik Harness: worn full-time for 6–12 weeks with ultrasound follow-up
6 Months to 2 Years
• If Pavlik fails or diagnosis is late:
• Closed Reduction under anesthesia
• Hip Spica Cast for several months
Over 2 Years
• Open Reduction
• Pelvic and/or Femoral Osteotomy to improve joint stability
Long-Term Outlook
Most children achieve normal hip function if treated early.
If untreated, DDH can lead to:
• Early osteoarthritis
• Gait abnormalities and leg-length discrepancy
• Avascular necrosis of the femoral head
Talib Chichan
Al-Mustaqbal University
The First University in Iraq.