

Anal Canal
29/04/2025 Share :
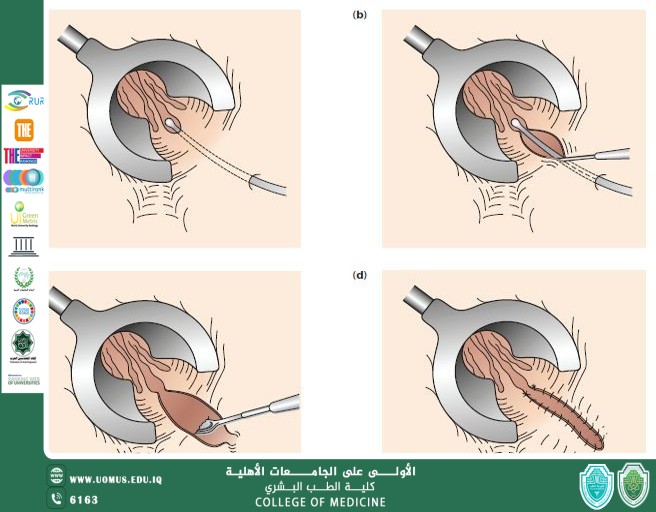
Final segment of GI Tract<br />Lies within Anal Triangle of perineum<br />Important role in defecation and Faecal continence<br />Surgical Anal Canal begins at the anorectal<br />junction and terminates at the anal verge.<br />Measures 2-4 cm in length.<br />Anatomic anal canal extends from dentate (pectinate) line to the anal verge.<br />Dentate line (Pectinate) marks the transition<br />point between columnar rectal mucosa and squamous endoderm.<br />Anatomy of Anal Canal<br />External Sphincter:<br />It is a striated muscle.<br />Under voluntary control<br />Supplied by pudendal nerve.<br />Has 3 segments Deep, Superficial, subcutaneous.<br />Its deep segment is continuous with the puborectalis muscle and forms the anorectal ring, which is palpable upon digital rectal examination.<br />Tonically contracted at rest<br />Internal Sphincter:<br />It’s a smooth muscle.<br />Under autonomic control<br />It is an extension of the involuntary circular smooth muscle of the rectum.<br />Totally contracted at rest but relaxes as a consequence of reflex activity, predominantly during defecation.<br /><br /><br />What is Fistula-in-ano<br />A fistula in ano or anal fistula, is a chronic abnormal communication, usually lined to some degree by granulation tissue, which runs outwards from the anorectal lumen (internal opening) to an external opening on the skin of perineum or buttocks.<br />Basically it’s an abnormal connection between anal canal and Perianal skin or we can say that it’s abnormal connection between two epithelialized surfaces.<br />More common in men<br />Common in third, fourth and fifth decade of life.<br />Pathophysiology<br />An anal fistula forms as a result of an anal abscess. An abscess is a collection of pus in an area of the body. An anal abscess develops when a small anal gland becomes infected with bacteria.<br />Anal abscess is by far the most common cause of anal fistula and up to half of all patients with an anal abscess will develop an anal fistula.<br />The formation of an anal fistula is more likely to occur if:<br />the abscess bursts before treatment<br />the fluid is not drained entirely<br />the abscess fails to heal completely<br />Etiology<br />Cryptoglandular hypothesis<br />History of anal abscess formation<br />Crohn’s disease<br />Smoking<br />Tuberculosis<br />Lymphogranuloma venereum<br />Actinomycosis<br />Foreign body<br />Immunocompromised conditions (HIV, malignancy<br />Classification<br />Intersphincteric fistula:<br />It is the result of a perianal abscess<br />The tract begins in the space between the internal and external sphincter muscles and opens very close to the anal opening.<br />Transsphincteric fistula.<br />this fistula results from an ischiorectal fossa abscess<br />The tract begins in the space between the internal and external sphincter muscles or in the space behind the anus. It then crosses the external sphincter and opens an<br />inch or two outside the anal opening. These can wrap around the body in a U shape, with external openings on both sides of the anus (called a horseshoe fistula).<br />Suprasphincteric fistula.<br />It arises from a supralevator abscess<br />The tract begins in the space between the internal and external sphincter muscles and turns upward to a point above the puborectal muscle, crosses this muscle, then extends downward between the puborectal and levator ani muscle and opens an inch or two outside the anus.<br />Extrasphincteric fistula.<br />may arise from foreign body penetration of the rectum with drainage through the levators, from penetrating injury to the perineum, from Crohn disease or carcinoma<br />The tract begins at the rectum or sigmoid colon and extends downward, passes through the levator ani muscle and opens around the anus.These fistulas are usually caused by an appendiceal abscess, diverticular abscess or Crohn's disease.<br />Patient Presentation (History)<br />PERIANAL DISCHARGE (Intermittent/constant or purulent/bloody)<br />PERIANAL PAIN (Worse during defecation, may be constant lump in perianal area)<br />BLEEDING IN PERIANAL AREA<br />PRURITUS around anus<br />DIARRHEA and ABDOMINAL PAIN (could suggest crohns)<br />FEVER<br />DISCOLORATION OF SKIN SURROUNDING FISTULA<br />Differential Diagnosis<br />Acute Proctitis<br />Constipation<br />Anorectal abscess<br />Diverticulitis<br />Inflammatory bowel disease<br />Anal carcinoma<br />Hidradenitis suppurative<br />Sexual abuse<br />Pilonidal cyst and sinus<br />Syphilis<br />Tuberculosis<br />Physical Examination<br />Examination under general anesthesia<br />Full examination/inspection of perineum<br />Check for any external openings<br />Any swelling<br />Palpate for pus/fluid<br />Palpate fistula tract<br />Abscess (tenderness)<br />Note other abnormalities (hemorrhoids, fissures etc)<br />Inject Hydrogen peroxide allows to visualise bubbled at internal openings<br />DRE: Area of induration, fibrous tract and internal opening may be felt<br />PROCTOSIGMOIDOSCOPY: To evaluate rectal mucosa for underlying disease process<br />Clinical Assessment<br />The key points to determine:<br />Site of the internal opening<br />Site of the external opening(s);<br />The course of the primary track<br />The presence of secondary extensions<br />The presence of other conditions complicating the fistula<br />Goodsall’s Rule<br />Indicate the likely position of the internal opening according to the position of the external opening(s)<br />The site of the internal opening may be felt as a point of induration or seen as an enlarged papilla<br />Imaging Techniques<br />Not performed for routine fistula evaluation<br />Can be used when primary opening is difficult to identify, or in the case of multiple or recurrent fistulae<br />Endorectal Ultrasound:<br />To help define muscular anatomy differentiating intersphincteric from transphinicteric lesions<br />MRI:<br />Becoming study of choice when evaluating complex fistulae<br />Treatment (Surgical Management)<br />Surgery is done to:<br />Prevent recurrent abscess<br />Cure fistula<br />Fistulotomy (lay open)<br />Fistulectomy<br />Setons<br />Mucosal Advancement Flap<br />Ligation of the Intersphincteric Fistula Tract (LIFT)<br />Fibrin Glue<br />Approach Consideration<br />Preoperative considerations include the following:<br />Rectal irrigation with enemas should be performed on the morning of the operation<br />Anesthesia can be general, local with intravenous sedation, or a regional block<br />Administer preoperative antibiotics<br />The prone jackknife position with buttocks apart is the most advantageous position<br />Intraoperative considerations include the following:<br />Examine the patient under anesthesia to confirm the extent of the fistula<br />Identifying the internal opening to prevent recurrence is imperative<br />A local anesthetic block at the end of the procedure provides postoperative analgesia<br />Fistulotomy<br />Make incision over an entire length of fistula using probe as guide.<br />Useful for 85-95% of primary fistulas (ie, intersphincteric, and low transsphincteric)<br />A probe is passed into the tract through the external and internal openings.<br />overlying skin, subcutaneous tissue, and internal sphincter muscle are divided with a knife or electrocautery, and the entire fibrous tract is thereby opened.<br />If the fistula tract courses higher into the sphincter mechanism, seton placement should be performed.<br />RISKS:<br />Creates larger wounds that take longer to heal and offers no recurrence advantage<br />Fecal incontinence may be present<br />Fistulectomy involves coring out of the fistula, usually by diathermy cautery<br />it allows better definition of fistula anatomy than fistulotomy<br />especially the level at which the track crosses the sphincters and the presence of secondary extensions.<br />This technique is useful in patients with:<br />Complex fistulas (ie, high transsphincteric, suprasphincteric, extrasphincteric) or multiple fistulas<br />Recurrent fistulas after previous fistulotomy<br />Anterior fistulas in female patients<br />Poor preoperative sphincter pressures<br />Patients with Crohn disease or patients who are immunosuppressed<br />Seton Suture CUTTING SETON:<br /><br />The seton is tightened down.<br />Intention of cutting through the enclosed muscle.<br />Used if fistulas are in high position<br />Minimising sphincter dysfunction due to least scar formation<br />LOOSE (DRAINING) SETON<br />Loose setons are tied such that there is no tension upon the encircled tissue<br />There is no intent to cut the tissue.<br />For long-term palliation to avoid septic and painful exacerbations<br />As part of a staged fistulotomy.<br />Preserve the external sphincter in trans-sphincteric fistula<br />Mucosal Advancement Flaps<br />When the sphincter complex is not too indurated and adequate intra-anal access can be obtained, the advancement flap technique can be employed<br />This procedure involves total fistulectomy, with removal of the primary and secondary tracts and complete excision of the internal opening.<br />A rectal mucomuscular flap with a wide proximal base (two times the apex width) is raised.<br />The internal muscle defect is closed with an absorbable suture, and the flap is sewn down over the internal opening; closing of the communication with anal lumen with an adequately vascularised flap<br />Advantages include a one-stage procedure with no additional sphincter damage.<br />Disadvantage is poor success in patients with Crohn disease or acute infection.<br />Ligation of the Intersphincteric Fistula Tract (LIFT) It is a sphincter-sparing procedure for complex transsphincteric fistulas<br />The technique involves disconnection of the internal opening from the fistula tract at the level of the intersphincteric plane<br />Removal of the residual infected glands without diving any part of the sphincter complex.<br />The tract is then ligated and divided, the internal part is removed<br />The external part of the track is curretted out and drained.<br />Hence it is a sphincter-preserving procedure<br />Fibrin Glue Only non surgical option for treating fistula<br />Fibrin glue is injected into the fistula to seal the tract<br />The opening is stitched closed after the injection<br />Poor long term results<br />"Al-Mustaqbal University is the first in Iraq."<br /><br />Dr. Maythum Alarajy<br /><br /><br /><br />